


Your Cardiologist is Blind
Smarter Statin Use- A Modern Approach
*This is not medical advice. It may or may not be as helpful as the advice you get at a doctor’s office.
By the time most men hit their 40’s their body is likely falling apart in some way. A joint hurts, the beer gut is too egregious to ignore, or funerals have gone from a rare occurrence to a relatively common one. As a result, you’ll end up at the local doctor whom you found on Google Search, or even better, your wife has let you know when your appointment is. They’ll take your blood pressure and medical history and if you’re lucky, begrudgingly order you an inadequate lipid panel to give off a spirit of control. Congratulations, you have just earned yourself a lifetime statin prescription.

At your local Walgreens or CVS you can pick up your Lipitor, or you if prefer a bit more spice, some Crestor. In a short 12 months, you will return back to go through the same motions.
Unbeknownst to you, your cardiologist may only have a rough idea of what that statin is doing to your body. If he’s lucky, in 12 months it will turn out that he has blindly prescribed you a dose that works well. If you’re unlucky, you’ve lived the past year with side effects you didn’t know were optional and worse, your risk of heart disease and heart attack have likely not decreased.
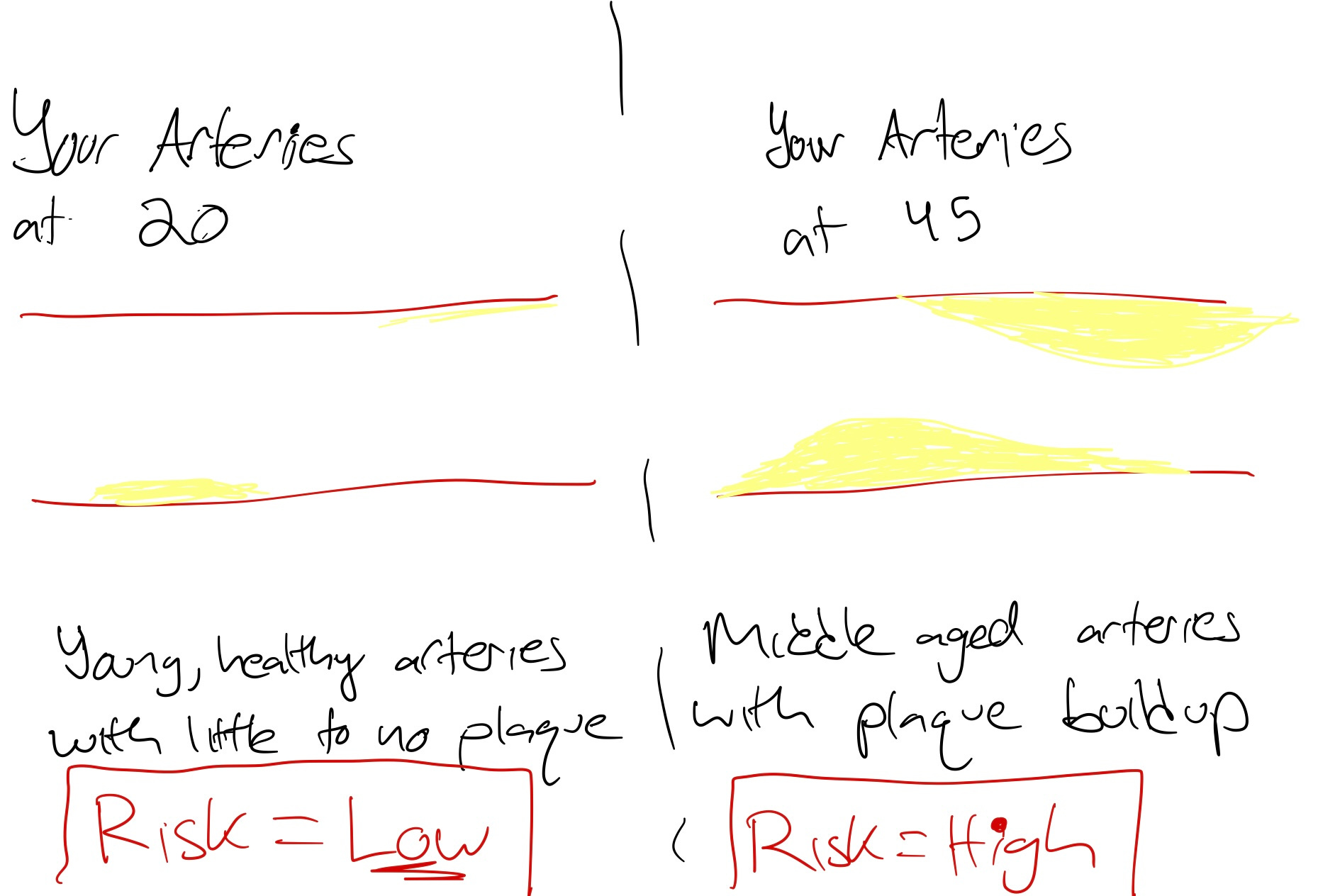
Plaque (the yellow in the image) in your arteries is a buildup of fatty deposits that restricts normal blood flow in your arteries, which can lead to heart attacks or strokes.
As you age and become “unhealthier” this plaque tends to build up. You typically won’t find a young man walking around with concerning plaque buildup. But as the decades roll on, this plaque commonly builds up in your arteries. This can be caused by a multitude of reasons that include cholesterol, smoking, diet, exercise, genetics, etc.
Statins are a common solution because they work by lowering cholesterol, thereby in a complicated way reducing new plaque formation in your arteries. Statins are therefore a common sense solution for many Americans, and carries a pretty low-risk factor.
It’s even estimated that 35% of Americans are on a statin. [Source]
The principal problem is that you and your cardiologist are simply guessing if the statin is working well.
I use an easy analogy below to display what is wrong with the typical use of statins from my POV.

Before: The house is slowly taking on some water damage to its structure, and even has a small amount of water inside the house! However, at a quick glance at your annual visit to the house, you notice the water building up outside.
As most would do, you quickly work to get rid of the water buildup outside. It’s too expensive and inconvenient to return to the house often, so you simply plug up the hole on the outside of the house and proclaim all is good at your checkup! At your next annual visit, you even notice some flowers have started growing outside.
After: While on the outside things are looking good, you’re in for big trouble in the long run. While you’ve plugged the outside hole with your generalized solution, you have caused detrimental downstream problems to your house. More water has ended up inside, destroying the first floor, and the house is crumbling. The convenience and general ease of plugging the outside hole left you with a false sense of security.
The way we prescribe and manage statins today is archaic. It is like plugging the small leak on the outside of your house whilst the foundation cracks and the insides flood. To improve your heart health, you must get inside the house and fix the foundation.
The incentives and traditions of your 60 year old well meaning cardiologist does not lend itself to you fixing your foundation.
The House and Your Body
Assessing the Culprit
The House: To say that the water damage is only a result of one small hole in the ground is ignorant of what’s going on inside your house. You must explore the foundation, your roof, and the basement.
Your Body: To say that heart attack risk is only a result of high LDL is ignorant of what’s going on inside your body. You must explore your metabolism, genetic risk factors (Lp(a)), and lifestyle
Determining your Solution
The House: 1. Fix the foundation, 2. pump the existing water out of your house, 3. fix the roof and 4. plug the holes in the ground
Your Body: 1. Fix your metabolic health, 2. exercise consistently, 3. eat consciously and 4. Take your statin
New Age Statin Medication
Baseline, Comprehensive Cardiovascular & Metabolic Panel
LDL, HDL, apoB, Trigylcerides, Lp(a) etc
Most importantly, we do not want to JUST know your LDL-C. This is utterly lazy, and the equivalent of searching for the easiest hole to plug in your yard. There is so much to explore in your body
We must know our apoB levels- this is the main cholesterol particle responsible for the build up of plaque. This is not a super common test handed out at your PCP.
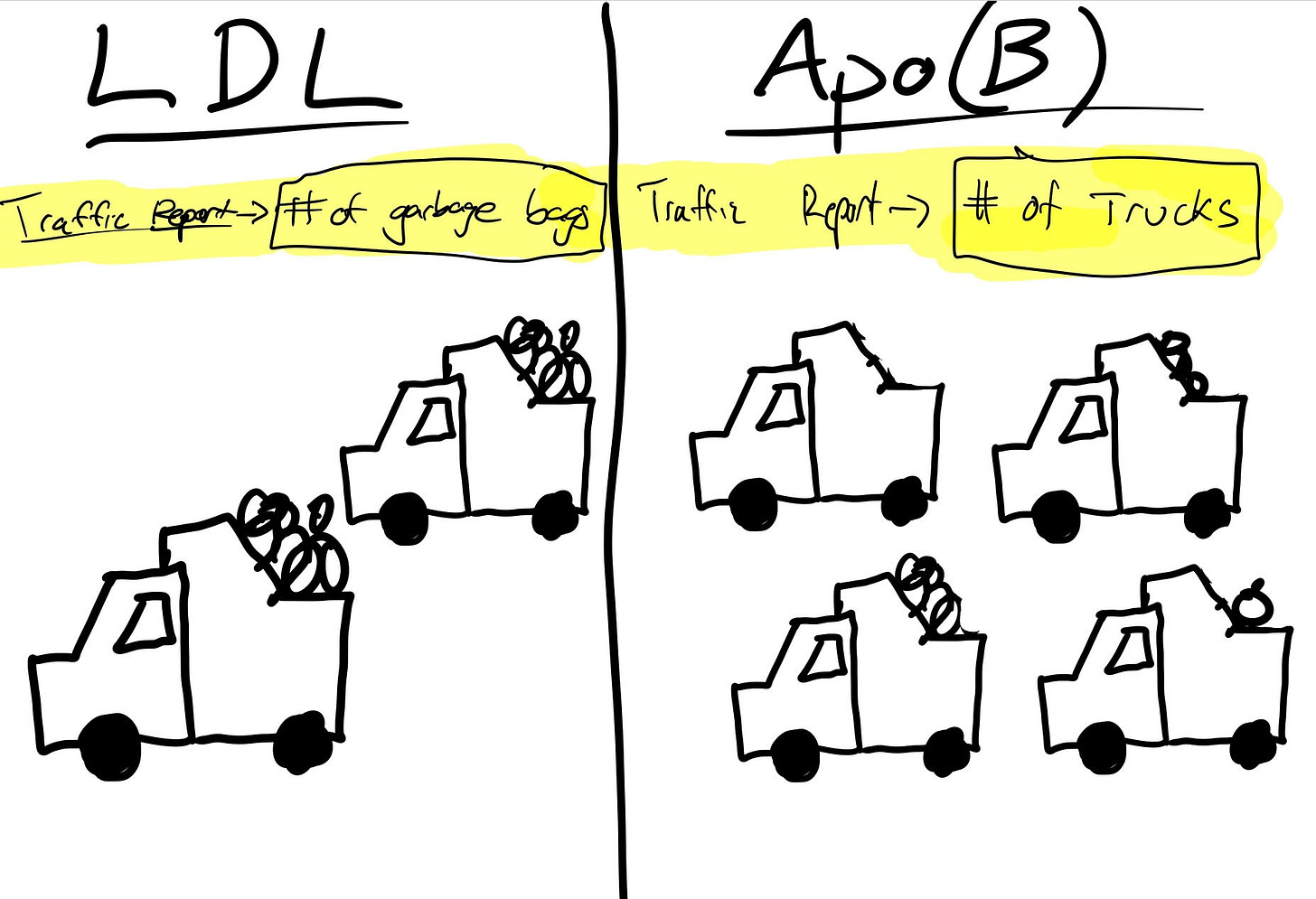
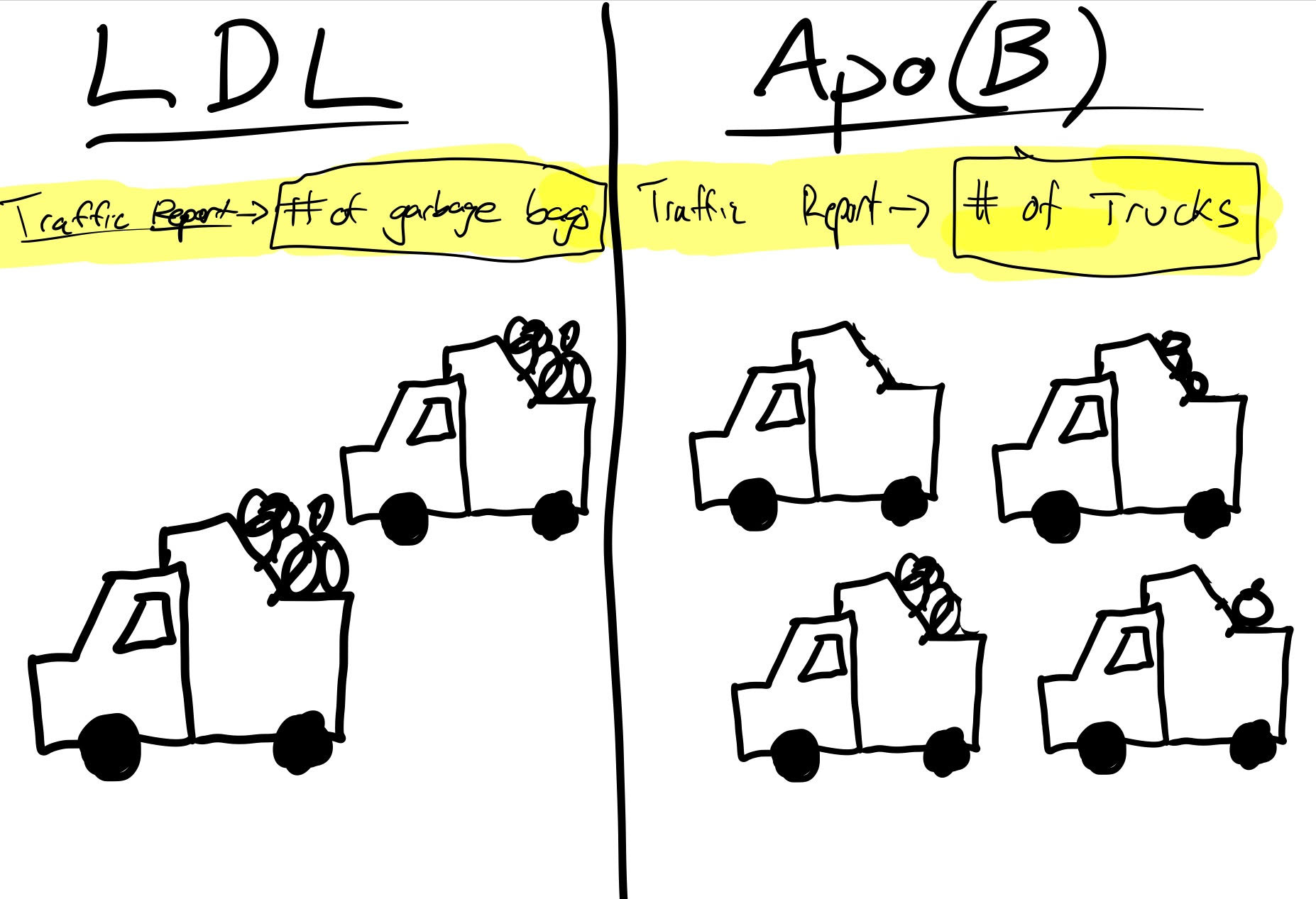
In the above illustration, we see the difference between measuring LDL and apo(B). When we measure LDL to determine cardiovascular risk, it is like measuring traffic by counting the number of garbage bags on the road. While more garbage bags on the road will likely mean more cars and more traffic, garbage bags don’t cause traffic.
Instead, counting the cars on the road is a much more accurate measure of cardiovascular risk, because cars cause traffic.
In this same way, measuring LDL is a way to approximate cardiovascular risk, just like counting garbage bags. It will give you a solid idea. But measuring apo(B) will tell us the number of “atherogenic particles” or particles that actually cause plaque buildup, and thus increase cardiovascular risk.
Stop just counting garbage bagsGet your low-lift lifestyle fixes in place
This might be getting 10k more steps per day for some, or simply choosing not to have the twinkie for dessert. However, we all need an assessment of how our lifestyle might be influencing our cardiovascular risk. Wherever you fall on the spectrum, the easiest thing to do is to take a proactive step toward the right end of the spectrum.
IF APPLICABLE: Start your Statin
Talk to an MD about what statin is best for you, and start with the lowest effective dose. (More on this in step 4)
Whilst we are making tremendous strides in our lifestyle, diet, and exercise, a low risk statin may be sensible to prevent the buildup of future plaque.
Re-Test your Cardiovascular and Metabolic Panel
By re-testing our biomarkers 6-8 weeks after initiating lifestyle changes and statin dosages, we can begin to see their effects. We are not going to wait a year to check you blood pressure and LDL to see if you *may* have some ancillary health measurements that are improving.
By measuring apoB and other applicable markers we will get data-driven feedback on if our statin dose is working.
No markers changing? Let’s up the dosage a little bit
Seeing great improvements but having some side effects? Let’s reduce your dose
I think of lifestyle changes and biomarker testing in two ways.
Lifestyle Changes: This is like frequently showing up to your house. We are able to make sensible improvements to our foundation which will pay off in the long-run. Before launching a massive construction project (statin) at our house, first we should make lifestyle changes and see if we can make an impact.
Biomarker Testing: This is the equivalent of going inside your house and periodically assessing the damage or success of your efforts taken outside.
Is your diet improving your HbA1c? Let’s find out and not guess!
Is your statin actually lowering your apoB and cholesterol? Lets find out and not guess!
While the headline of this piece is drastic, it’s simply a reality that most cardiologists are ill-equipped or incentivized to go under the hood with you to manage your statin correctly.
We have been working diligently at SiPhox to fix this with our Cardiometabolic Program. Our at-home tests allow you to take care of these biomarker panels without shelling out a few grand to LabCorp or arguing with your Doctor about what labs are necessary. Our clinical team is then capable of strategically and analytically giving you a personalized statin dose for whatever duration might be appropriate.
This is not a quick doctor’s visit and a “see you next year”.
We’d love to help you rebuild your foundation.
https://home.siphoxhealth.com/programs/heart-health